Annual LPC Conference 2023: Resources
Published on: 31st October 2023 | Updated on: 31st October 2023
This year’s Annual LPC Conference was held on 13th October 2023 and marked an important event following the launch of a ‘Vision for Community Pharmacy’ and the changes in the LPC network, including the rebrand of LPCs to Community Pharmacy <Local>.
In total, more than 100 LPC representatives met in London, representing 48 out of 55 LPCs. Additionally, LPC representatives were joined by representatives from Community Pharmacy England.
Meeting sessions
The conference discussed a range of issues facing the sector. Community Pharmacy England CEO, Janet Morrison, gave an update about the current negotiations for the Community Pharmacy Contractual Framework 2024/25. Assistant Director of Digitising Primary Care – NHSE Transformation Directorate, Charis Stacey, talked about digital developments relative to the Primary Care Recovery Plan.
Governance Consultant, Victoria Finney, briefed delegates about the new draft Governance Framework and Code of Conduct for Community Pharmacy England and LPCs. Similar to last year, this year’s conference also held a Soapbox session. Lastly, LPC representatives engaged in group discussions and had the opportunity to ask questions to the Leadership Team.
In the link below you can find links to the agenda and conference papers, slide deck and Slido report:
Soapbox
Similar to last year, the 2023 LPC Representative Conference held a Soapbox session. This section of the agenda gave participants an opportunity to feed in topics and issues via Slido, which could be rated by the other attendees. The 3 most popular contributions where then elaborated on-stage.
This year, participants were eager to further hear about the following 3 issues that didn’t make it on to the main agenda:
- Push for walk in (rather than referrals) for future services like Pharmacy First .
- Community Pharmacy is in a workforce crisis – how can we all work together more effectively at all geographical levels to maximise support for pharmacy workforce, creating parity across primary care?
- Operational delivery of IP Pathfinder – exploring operational aspects to support the pharmacies to make the pilot services a success.
Wider Participant Engagement
Throughout the event, attendees could participate and engage with each other through group discussions, Q&A with the Community Pharmacy England Team, Slido polls and further commentary functions on the Slido platform.
Group Discussions
LPC Representatives discussed key aspects of the Vision and the way forward in terms of implementing it. There were many robust points mentioned. Below is a summary of the key points raised. A full read out of the notes can be accessed here.
Have you done anything with the vision locally so far – what has worked well, and what has been the reaction?
- Highlighted the need for LPCs to understand the Vision report first.
- Initial reactions indicate that the Vision report has not been fully digested yet, but it has been flagged to key stakeholders and local leaders.
- Several attendees mentioned they were already implementing action points from the Vision before its official launch.
- Mixed response from local MPs, with no response from some, indicating a need for more engagement.
- Some negativity observed regarding why the ICSs have all the actions.
- Several LPCs have introduced the Vision to local ICS’ with a positive initial reaction.
- While well presented, nothing exceptionally new in the report.
- Emphasis on the need for a long-term approach.
- Positive feedback on the summary of the Vision and the use of animations.
- Some LPCs have shared the Vision documents and strategies for local sharing.
- Specific example from Lincolnshire about sharing Vision information and collaborating with a local university on a wellbeing service.
How do you think local systems will feel about their suggested actions – what can LPCs do to encourage and help them to take those actions?
- Local systems are currently reactive and focused on existing pressures.
- Clarity needed that it is a 10-year plan and not all resources must be available immediately. Concerns about the feasibility of communicating the entire plan at once.
- Worries about community pharmacies being pushed onto ICS without sufficient resources.
- Recognition of structural inequalities among LPCs and ICBs of different sizes.
- Suggestions to involve ICS’s in wider targets such as lobbying efforts and infrastructure.
- Consider stimulating innovation among contractors for quick wins.
- Suggestion for CPE to provide LPCs with a checklist for available resources and tracking actions.
- Challenges with merged LPCs still working independently instead of collaboratively.
- The importance of closer working relationships with LRCs and LMCs.
- Concerns about funding and resources due to recent changes in the levy.
- Acknowledgment of weak relationships between GPs and Community Pharmacies, emphasizing the need for improvement. Often a GP focused approach by ICBs.
- The importance of a bottom-up approach to building constructive GP-pharmacy relationships.
- Tensions arising from the battle for service provision, such as flu jabs and CPCS.
- Positive progress in London and within regional taskforces, although it can be slow.
- The effectiveness of Pharmacy London in facilitating collaboration.
- The challenge of change taking 3-5 years, potentially conflicting with NHS reforms.
- Emerging closer collaboration between Public Health and ICBs.
- Limited focus on patient experience at the local level due to constraints.
- Issues noted with the smoking cessation service and lack of trust referrals.
- The need to connect the asks in the Vision to Fuller action.
- Recognition that some are starting to see Primary Care as an essential tool for engagement.
How should local Government be engaged – can they help us?
- Engagement with Local Government – Concerns regarding the integration of public health services and the influence of external companies that have won tenders in sector conversations
- Challenges in Engaging Local Officials – Concerns raised about attitudes and motivation of local officials to engage with Community Pharmacy interests. LPCs should interact with local officials in the same way they engage with MPs.
- Consensus that local councillors have more power and influence than previously assumed.
- Collaborating with LMC for primary care service commissioning provides a stronger position.
- The government could help change the perception of pharmacies, emphasizing their role in delivering clinical services alongside medicine collection.
- Key partners for engagement – Healthwatch and the PNA group were identified as key partners. Polling patient experience was seen as an effective way to send a strong message.
- It was noted that patient-led pressure can have more impact than MPs.
- MP visits were seen as important opportunities for engagement, as they can listen and ask questions. MPs may be swamped, but engagement is crucial to maintain or establish relationships.
- Suggested potential engagement with Directors of Public Health, Health and Wellbeing Boards (HWB), and scrutiny committees to brief them on the vision.
How should LPCs take forward the vision at a local level – can you identify specific ideas and actions?
- Enhance collaboration through regular meetings and forums for healthcare providers, standardised communication protocols, systems to facilitate data exchange and joint training and education programmes to foster interdisciplinary collaboration.
- Streamline processes through identifying and eliminating redundant administrative processes that hinder efficiency, develop shared electronic health records and information systems for seamless patient care and stablish clear referral pathways and guidelines to facilitate patient transitions between providers.
- Create incentives and recognition programs for healthcare providers who actively participate in collaboration efforts. Implement shared quality metrics and outcome measures to assess and reward successful collaboration.
- Strengthen inter-organisation governance through developing clear agreements and protocols for decision-making and dispute resolution and promoting a culture of shared leadership and responsibility for collaborative efforts.
- Explore telemedicine and remote monitoring solutions for coordinated care.
- Ensure data security and privacy measures when sharing patient information.
- Establish mechanisms for ongoing assessment and feedback to identify areas for improvement.
- Encourage a culture of continuous learning and adaptability among healthcare providers.
- Foster research and development collaborations for innovative healthcare solutions.
What resources do LPCs need and how can they support national work to take forward elements of the vision?
- A platform for sharing successful strategies and initiatives.
- Fundamental principles for commissioning need to be agreed upon across regions, if not nationally.
- The promotion and dissemination of animations and comprehensive resource packs for use with local stakeholders.
- Consider changes in the structure to make it more pharmacy-led, such as transforming CPCS into a walk-in service that’s not solely dependent on GP referrals.
- Addressing the biggest barrier of IT integration to ensure seamless data sharing and communication.
- Establishing better mechanisms for the flow of information and collaboration.
- Development of template letters and emails by Community Pharmacy England to assist LPCs in conveying the most important points and key takeaways from the Vision report.
The Community Pharmacy England Leadership Team answered a wider range of questions from LPC representatives. Attendees could post questions on Slido and rate each other’s input. The most popular questions were answered in plenum. You can read the Q&A session below.
Q&A with Leadership Team
Q1) Have we challenged paymaster to improve speed of payments for clinical services activity? Cashflow impact on last minute Covid/flu (workforce/product) is dire?
Mike: The short answer is yes. We have talked to the NHS BSA and pushed for the system to be more efficient and user friendly. This is something that is being worked on and more updates will follow.
Q2) Branded prescribing of Physeptone instead of generic way above DT by CGL… any collective action being planned to help those contractors who are heavily reliant
Mike: This is a specific example of a larger problem. There have been ongoing attempts to address this issue over the past 15 years without a solution Specifically to methadone, the issue will be addressed in further detail at the next CLOT meeting. It would be helpful Mubasher could send in his question in more detail to make sure that it properly addressed at the next meeting.
Q3) Could contractor survey results be broken down into local CPLs. It would be great to hear what local CPs are telling CPE so we can further support at local level.
James: We are continuously working on innovating our polls. Based on the data we have now we are able to break down 1 out of 3 segments on the LPC level. Further to our developments of the poll, we are currently creating a dashboard which will soon become available. We are also incorporating LPC feedback into our ways of innovating the poll.
Q4) When is the £645million recovery plan coming out, contractors are drowning?
Janet: It is too early to say when the £645 million will be delivered. We have an aspiration that the money for the expansion of the BP and contraception services would come out sooner, if the rest is coming out later. There hasn’t really come much out of this, so in sum it cannot be concluded when the money will be delivered.
Q5) Is the new Common Ailment service going to be a walk in service?
Janet: It is a walk-in service, but is connected to the other referral pathways.
Q6) Can CPE and CPLs work with NHSE and ICBS to develop a Quality Commissioning Framework to prevent poor commissioned services e.g. DMS and CP IP Pathfinder?
James: We have given your feedback to NHSE and there is no appetite from the NHS to adopt a commissioning framework. We should rather focus on making better use of the tools that are already available e.g the National Enhanced Service routes.
Q7) Given the supply challenges that Branded Generics give us, is there a push for Generic substitutions for medicines not recommended to be prescribed by brand?
Gordon: There is no push for generic substitution at the moment. But there is a push for pharmacists to have more discretion for changes for formulations and other aspects.
Q8) Will the next CPCF be tiered for those CPs which are progressive?
Gordon: The short answer is no. Based on the current model there is a universal contract for contractors, and then there are additional contracts which should be viewed as complimentary to the universal one.
Q9) Will there be protection for bricks and mortar pharmacies in contrast to DSPs?
Gordon: We do support provision of services remotely, where it is appropriate to do so clinically. We recognise that DSPs can undermine the integrity of the market entry system. The solution too this is complicated and has been on the agenda over a longer period of time. Updates on this issue will follow in due time.
Q10) Will the next CPCF be tiered for those CPs which are progressive and will there be protection for B&M pharmacies in contrast to DSPs?
Janet: A quick reflection is that caps are problematic for several reasons, as there may be several unintended consequences for that. The issue will be brought forth to the committee, who will consider this in further detail.
Q11) Can the LPC Representatives Conference be a hybrid event next year?
James: This year’s conference was an all in person event based on the overwhelming feedback from last years’ attendees. The answer to this question is conditional to the feedback from this year’s conference. We will also discuss the feedback from this year’s event at the next CLOT meeting.
ICB
Attendees were asked to rate their attitudes toward engagement with their local ICB, on a scale from 1-5 with 5 being the most positive. The poll results are skewed towards positive attitudes towards engagement with their local ICB.
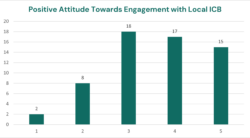
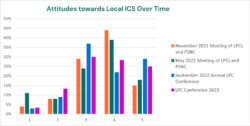
We have also tracked LPC representatives’ attitudes towards engagement with their local ICB. Trends can be seen in the charts below.
Operational Delivery of the IP Pathfinder – Ideas to make it the golden bullet of change in the sector
Participants were asked to feed in their thoughts on the operational delivery of the IP Pathfinder, with the aim of making it the golden bullet of change in the sector and how LPC can help in this process. Below is a summary of what ideas came through.
Summary from LPC Representatives Input
Workforce and Technology Enhancement:
- Free up the pharmacist with workforce and technology
- Request local practices to consider recruiting IP Pharmacists
- Hub and spoke at the national level, techs running dispensing
- Need to expand the workforce with attractive offers
- Funded training courses for pharmacy staff
Funding and Financial Support:
- Need to support with funding IPs
- LPC support contractors being able to access IPs
- Funding 2 consultation rooms and 2 pharmacists
- Clinical checks, broader use of accuracy checkers
- The answer is within our own knowledge and workforce
Interprofessional Collaboration (ICB and ICS):
- Agree and work with ICBs on funding applications
- Secure ICB lobbying for parity of resources
- Utilization of the whole team with delivery of services
- Full flexibility at a local level for implementation
Pharmacy Technician Empowerment:
- Let the techs run the pharmacy
- More ACTs, but pay them a better wage
- Upskilling techs and teams to support prescribing
- Enhance the skill mix and availability of other pharmacy team members
IP Pathfinder Development and Coordination:
- A register of IPs and those able to support with training and mentorship
- Mapping of IPs
- Identify IPs in their patch
- Work as a team with all involved
- Coordination of clinical supervisors for training
Information Technology and IT Infrastructure:
- National group sharing what’s working well and not working
- IP-based services require better IT
- Equity of access to training
Service Quality and Patient Experience:
- Shared patient budget to all IPs
- Related services universally available
- Stop doing it on the cheap
Maximising support for pharmacy workforce, creating parity across primary care
Attendees were asked to feed in their ideas on how we can all work together more effectively locally, regionally and nationally to maximise pharmacy workforce creating parity across primary care. Attendees fed primarily in ideas that could be categorised as either resource strategy or engagement. Their input is listed below:
Resources Strategy
- Clear national strategy on resource
- Share local implementation
- NHSE&I funded pharmacy technician apprenticeship
- Training hubs, staffing pools able to move between
- Workforce strategy
- Lobby for hiring a freeze in PCN/GP sites
- Need better return to afford the wages demanded
- Resources
Engagement
- Positive engagement
- Inclusive
- Supportive
- United
- One voice
Governance Framework
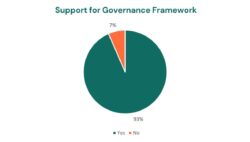
Governance Consultant Victoria Finney updated the Conference about the ongoing work on the governance framework. As part of this session, delegates were asked whether they could in principle support the framework, and code of conduct, subject to final refinements. An indicative poll took place via Slido, with an overwhelming majority supporting the way forward.
Can you support in principle the Governance Framework and Code of Conduct as relevant and appropriate for Community Pharmacy England and LPCs?
Participant feedback and the LPC Representative Conference 2024
The Conference of LPC Representatives is an event shaped by LPC representatives and for LPC representatives, facilitated by Community Pharmacy England. This means that Community Pharmacy England aims to provide a safe and convenient space for LPC representatives to engage. We are eager to hear your feedback and continue to accommodate your preferences as far as practically possible.
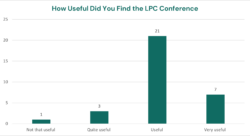
For this year’s conference, attendees reported a high level of satisfaction.
For the next conference we take on the feedback provided by our attendees. So far we have the following feedback on what LPC Representatives wish to see more and less of:
In future conferences LPC Representative wish to see more of:
- NHS speakers w Q&A sessions.
- Soapbox
- Network opportunities
- More opportunities to engage
- Table discussions
- Confidential CEO briefing
- CPhO
- Ongoing updates on the Vision – tie into CPE strategy
- ICB updates – possibly using NHS Confed (or similar) to share best practice
- More external stakeholder sessions – Fuller session was useful
- Work around practical joint operations
LPC Representatives with to see less of:
- Revisiting information already released
Further comments from LPC Representatives via Slido
Engagement and Preparations
- We should lay out some expectations to ensure attendees have read any documents that are being discussed at the conference
- Suggest conference working group is made up of all LPCs on a rolling programme of a small working group (maybe alphabetically), so all have to contribute and design
Guest speakers and content
- Would like to see ministers from the Government attending and explain their strategy for the sector.
- The soapbox needs to develop into motions to the conference to provide CPE with a mandate from contractors.
Location and facilities
- The LPCs that come from afar should have their accommodation paid for the night before to facilitate their attendance.
- Better audio facilities.
- I don’t support having hybrid meetings it needs to be one or the other.
- London is an easier venue than some more central locations. Depends on train links etc.
- Would prefer F2F conferences perhaps in Birmingham and London and alternative between the two.
- Birmingham please!
- In person works well
- I think a face to face approach is best. Happy for this not to always be London-based.
- In the interest of saving the LPC money having online or hybrid gives options
Positive feedback
- Great conference this year. I felt that things are moving in a positive direction for the future.
- Food was really good. Thank you
- Lovely to see everyone face to face. Venue was good, Comparing excellent, running of the meeting as a whole behind the scenes excellent. Well done to all involved and thank you!
- Soap box worked well for highlighting issues
Duration
- If it were to be a 2 day conference, contractors would need to fund that. I’m not sure that would be right.
- 2 day conference to include more input into negotiable positions, service development and policy. Move conference around all regions.
- I don’t support 2 days and that isn’t inclusive to working parents.
Further comments from LPC Representatives received offline
- You are building a really positive community among the CPLs
- Thank you all involved in delivering a valuable event today. Dr Fuller’s presentation was particularly well received .
- The conference went well yesterday. Thank you to the team for organising it so well.
- Great conference yesterday – thank you!
- Good conference and hope you have a good day








